https://www.frontiersin.org/articles/10.3389/fimmu.2020.552909/full
Otan tästä artikkelista niitä kappaleita sitaattina, joissa MERS kuvataan.
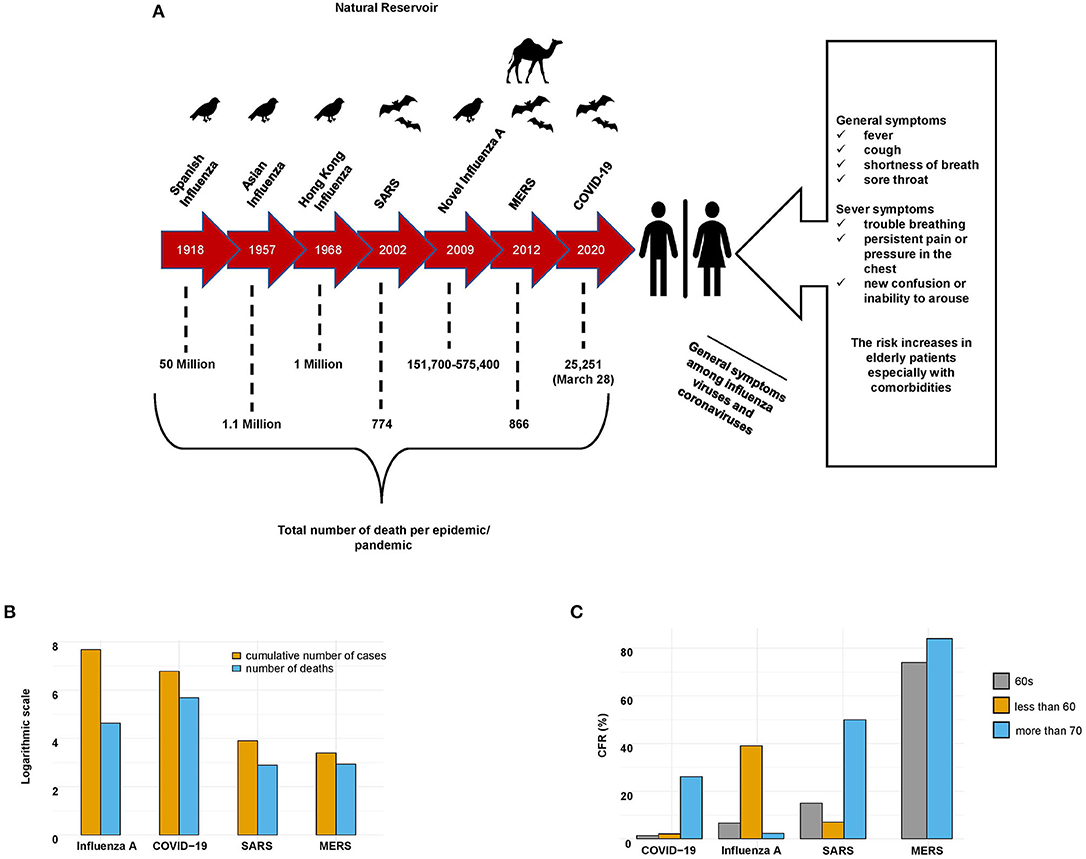
Kuva 1 vertailee ajallisesti purkauksia ja myös kuolleisuutta verrataan. prosentuaalisesti tautitapauksista.
{kind=link}
MERS-CoV
Although MERS-CoV belongs to the same family, order, and genus as SARS-CoV, it was the first betacoronavirus lineage C member identified as a “novel coronavirus” with a genome size of 30,119 nucleotides. The genome of MERS-CoV encodes 10 proteins. These 10 proteins comprise two replicase polyproteins (ORF1ab and ORF1a), four structural proteins (E, N, S, and M), and four nonstructural proteins (ORFs 3, 4a, 4b, and 5) (32). In addition to the rep and structural genes, there are accessory protein genes interspersed between the structural protein genes that may interfere with the host innate immune response in infected animals (7).
MERS-CoV
Unlike the SARS cases, most of the MERS cases had previous contact with dromedary camels. The MERS-CoV strains isolated from camels were almost identical to those isolated from humans (47, 48), and the MERS-CoV isolates were found to be highly prevalent in camels from the Middle East, Africa, and Asia (49, 50). Genomic sequence analysis indicated that the Tylonycteris bat coronaviruses HKU4 and HKU5 are phylogenetically related to MERS-CoV (they are all representatives of betacoronavirus lineage C) (51). Generally, all of the related MERS-CoVs isolated from bats support the hypothesis that MERS-CoV originated from bats (Supplementary Figure 1) (46).
Receptor binding viruses
The MERS-CoV spike protein subunit S1 C-domain has also been identified as the RBD (73).
However, unlike SARS-CoV, MERS-CoV uses a dipeptidyl peptidase 4 (DPP4)
β-propeller as its receptor. Likewise, the RBD of MERS-CoV contains an
accessory subdomain that functions as the receptor-binding motif (RBM).
Although the RBD core structures are remarkably analogous between
MERS-CoV and SARS-CoV, their RBMs are distinct and may result in the
recognition of different receptors (Supplementary Figure 2) (73).
Host factors, disease severity, and pathogenesis
Once a patient is infected with SARS-CoV, MERS-CoV, or SARS-CoV-2, the host innate immune system will identify the virus by using pattern recognition receptors (PRRs) , such as a toll-like receptor (TLR) , NOD-like receptor (NLRs) , or RIG-I-like receptor (RLRs), to recognize pathogen-associated molecular patterns (PAMPs).
The adaptive immune response also plays a significant antiviral role by stabilizing the host defense mechanism against pathogens and minimizing the risk of developing an autoimmune reflex response or inflammation (9, 79).
In general, human coronaviruses can be classified into two types: lowly pathogenic and highly pathogenic. Viruses with low pathogenicity, including HCoV-229E, HCoV-OC43, HCoV-NL63, and HCoV-HKU, can cause mild upper respiratory tract infections. In contrast, highly pathogenic viruses, including SARS-CoV, MERS-CoV, and SARS-CoV-2, can cause lower respiratory tract infections, severe pneumonia, and sometimes fatal acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), especially in older individuals (≥65 years old) (Figure 1C) (80).
In addition to the lungs, coronavirus infection may damage other organs or tissues, including the gastrointestinal tract (81), spleen, lymph nodes, brain, skeletal muscles, thyroid, and heart (82, 83). The destruction of lung cells prompts a local immune response, engaging macrophages and monocytes that respond to the infection, release cytokines, and enhance adaptive T and B cell immune responses. In some cases, a dysfunctional immune response occurs, which can cause severe lung and systemic pathology. The invading coronavirus may incite host immune responses, and an excessive immune response may cause immunopathological damage (known as a cytokine storm) in patients with coronavirus infections (9, 84). Cytokine storms may enhance the infiltration of non-neutralizing antiviral proteins that facilitate viral entry into host cells, leading to increased viral infectivity (82, 85). Therefore, cytokine storms play a key role in the pathogenesis and clinical outcomes of patients with coronavirus infection.
Transmissibility
SARS-CoV, MERS-CoV, and SARS-CoV-2 can survive on surfaces for extended periods, sometimes up to months. Like the influenza A viruses, the factors affecting the survival of these viruses on surfaces include the strain variation, titer, surface type, mode of deposition, temperature, humidity, and method used to determine the viability of the virus (98, 99). Several studies have indicated that SARS-CoV, MERS-CoV, and SARS-CoV-2 can survive on dry surfaces for a sufficient duration to accelerate onward transmission. Viable MERS-CoV was detected on steel and plastic surfaces after 48 h at 20°C with 40% relative humidity, with a decreased viability of about 8 h at 30°C with 80% relative humidity and of about 24 h at 30°C with 30% relative humidity. The estimated half-life of MERS-CoV ranges from ~0.5 to 1 h (98). On the other hand, another study conducted on the viability of SARS-CoVs detected on plastic surfaces and on polystyrene Petri dishes revealed that the virus survived for more than 5 days and more than 20 days, respectively, at room temperature. The viral viability was constant at lower temperatures (28°C) and lower humidity (80–89%) (100), whereas survival times ranged from 5 min to 2 days on paper, disposable gowns, and cotton gowns (99).
--
The effective management and control of such infections are increasingly performed with extensive contributions from mathematical modeling, which not only provides information on the nature of the infection itself but also makes predictions about the likely outcome of alternative courses of action (102). One useful mathematical model is the reproductive number R0, which is defined as the average number of secondary cases generated per typical infectious case (103). A value of R0 > 1 indicates that the infection may persist or grow in the population, whereas a value of R0 < 1 indicates that this infection will decrease in the population, although exceptions occur (103). The majority of seasonal influenza R0 values have been calculated for different populations and different continents, such as Europe and North America, with a median point estimate of R0 = 1.27 (IQR: 1.19–1.37) (104). The initial estimations of the reproduction numbers of SARS-CoV and MERS-CoV were calculated for China and the Middle East with R0 median = 0.58 (IQR: 0.24–1.18) (105) and R0 mean = 0.69 (95% CI: 0.50–0.92) (106), respectively. However, among the four viruses, SARS-CoV-2 has been calculated to be the most contagious, such as the R0 value associated with the Italian outbreak with a median point estimate of R0 = 3.1 (coefficient of determination, r2 = 0.99) (107).
Prevention, control, and treatment of infection
--
Since 2012, 27 countries have reported cases of MERS; Saudi Arabia has reported ~80% of human cases, and more than 50% of the cases in healthcare workers were nurses (115). The WHO, in collaboration with the Food and Agriculture Organization of the United Nations (FAO), the World Organization for Animal Health (OIE), and national governments, have been working with healthcare workers and scientists in affected countries to gather and share scientific evidence based on the previous coronavirus epidemic. This information gathering process has been beneficial for better understanding of the virus and the disease it causes and for the regulation of outbreak response priorities, treatment approaches, and clinical management tactics (113).
Although accumulated knowledge and risk preparedness from the influenza pandemics and SARS/MERS epidemics allowed researchers to examine the effectiveness of strategic plans in dealing with the ongoing pandemic of COVID-19, several challenges have been raised in preventing the spread of COVID-19, such as the lack of medical supplies and laboratory facilities for the assessment of the disease and the presentation of a high number of asymptomatic cases...
Generally, each pandemic/epidemic has presented a public health emergency of uncertain scope and effect; thus, essential elements of current approaches to pandemic preparedness and extenuation, such as the development of vaccines and stockpiling of antiviral drugs, necessitate detailed virological and immunological data on viruses with apparent pandemic potential. However, the development of vaccines against new strains is challenging. Therefore, physicians and health workers have found themselves facing the massive challenge of preventing infections or stabilizing patients' conditions. Thus, several promising attempts have been made to utilize different antiviral treatments that have already been approved by the U.S. Food and Drug Administration (FDA) for the treatment of viral pneumonia infections. A list of antiviral drugs and vaccine approaches for influenza viruses, SARS-CoV, MERS-CoV, and SARS-CoV-2 that have been used in clinics or are undergoing clinical trials are summarized in Table 2.
Inga kommentarer:
Skicka en kommentar